
Imagine this for a moment. You have been experiencing some unsettling symptoms and are struggling to know what is real and what is not. Your friends and family convince you to get some help, and you go to a local behavioral health organization where you are prescribed a medication that falls into the Second-Generation Antipsychotics (SGA) category1. This drug helps with your with your symptoms and allows you to feel some sense of normalcy, however, you are now experiencing symptoms of diabetes. A scary situation resulting in a trip to the ER confirms that you do, in fact, have Type 2 diabetes, and it could be a side effect of the medication you’re on. Now, you need both behavioral and physical health care regularly and could face severe health consequences or premature death. That is a lot of serious life changes to manage, and it is hard to imagine how there could be an approach to this in which anyone wins.
While this may not happen to everyone, it is not an unusual situation. It is estimated that people on SGA medications have at least twice the risk of developing Type 2 diabetes2, and the World Health Organization reports that people with severe and persistent mental illness have a staggering 10- to 20- year reduction in life expectancy compared to the general population3. Reasons for this include medication side effects, barriers to accessing treatment, physical inactivity, and high rates of tobacco or alcohol use.
In the past, behavioral and physical health care were kept separate in the treatment world. This resulted in people bouncing between providers with little communication about overlap in conditions. Now, funding sources, governing bodies, and regulatory agencies are incentivizing models of coordinated care to address this issue. So how does a system set up to be very one-dimensional shift to incorporate other disciplines? Frameworks4 for integration typically include care coordination and care management as part of the solution.
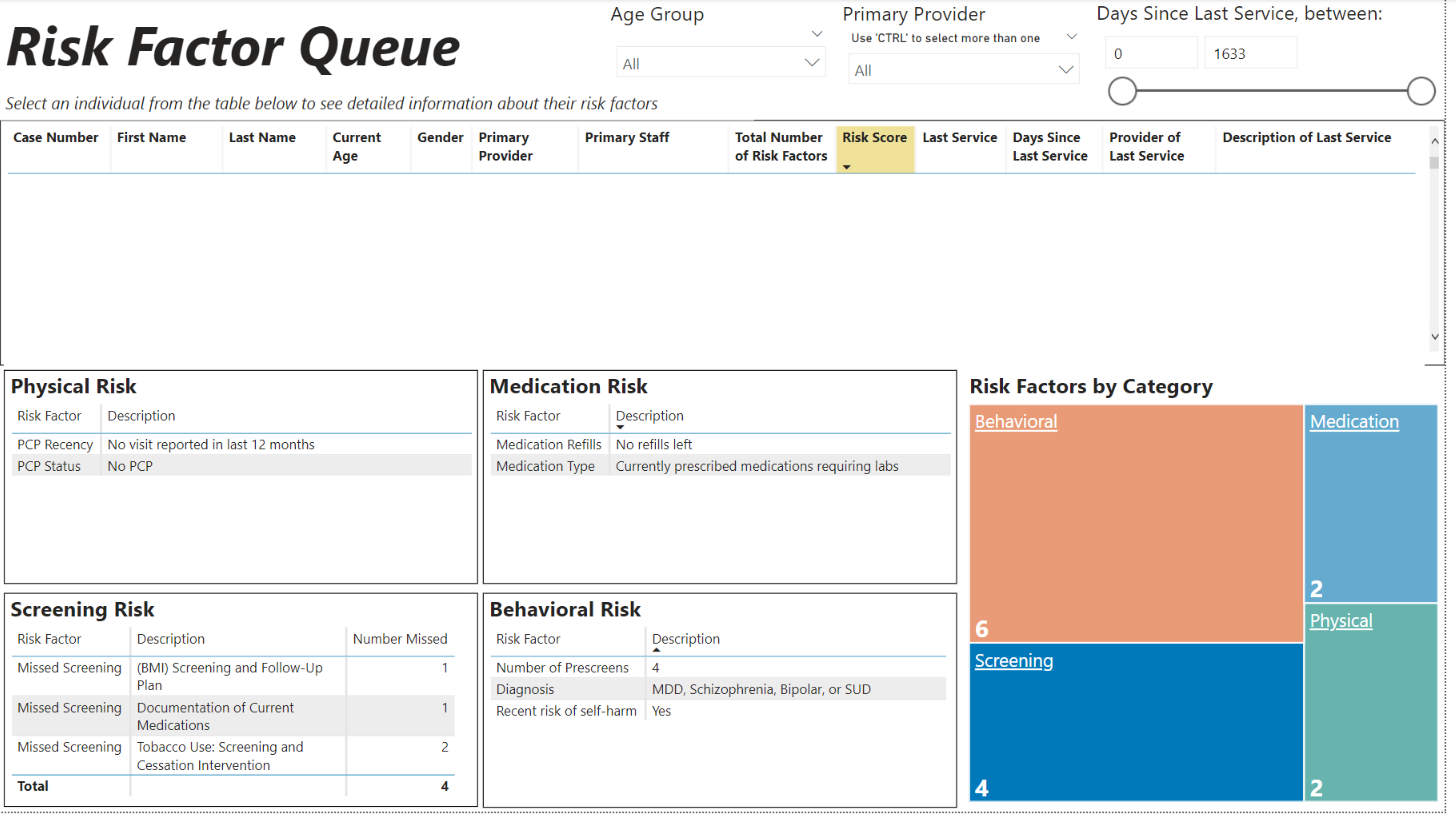
How do we incorporate framework into real life– particularly in this era of staffing shortages and red tape? Companies have to get creative in developing successful care coordination strategies. TBD Solutions recently worked with a CCBHC to create a system that utilizes data to assist care coordinators (sometimes called care managers, case managers, etc.) in prioritizing need. The Risk Factor Queue uses documents in a person’s chart to identify potential risk factors and calculate an overall risk score. Risk factors are categorized into physical, behavioral, and medication-related buckets. Complexity of need increases as the number of identified risk categories increase.
In our earlier example about developing Type 2 diabetes, you would have, at minimum, risk factors noted for your diagnosis and your medications, resulting in a score that is higher due to its complexity. The care coordinator does not need to read through your chart to find all the areas you may need help managing; it is readily available in one spot. Now they can use that information to inform decisions and discuss potential care needs with you. A conversation might look like this,“You don’t have a primary care physician on record? Let’s get you set up with one. You are out of refills on your prescriptions? We will make an appointment to review your medications and refill what is needed.”
Integrated care doesn’t require people to have expertise in behavioral and physical health care practices, but it does require that processes and systems be put in place to address the clear relationship between physical and behavioral health. Creative solutions must be developed to meet specific needs and incorporate the organization’s strengths. In this case, the need for efficiency from all involved parties was addressed. The care coordinator doesn’t have to spend as much time digging for information in the hopes, they are not missing a client5 who could benefit from their service, and you (the client) aren’t trying to manage your complex needs alone. This is a win-win-win in the eyes of the client, the care coordinator, and the continued quest for integrated care.



