
If you ask my friends and family to describe me, “organized” is usually the first word that comes up. I’ve always loved bringing order to my world. As a kid, I kept a clean and tidy room. Every toy, knick-knack, and item of clothing had a place and was never left out. I valued tidiness so much that I would clean my (less than organized) sister’s room for her. I completed my homework at the start of an evening or weekend, and if I had a large project, I had it done ahead of schedule. My organization skills reached peak performance when I became a wife and mom of three, now responsible for managing a household with seemingly never-ending laundry, cleaning, and shopping responsibilities.
At the root of my passion for order is my desire to feel prepared. Systematically assembling my space, structuring my time, and planning my activities gives me confidence and peace of mind. But here’s the catch: preparation alone isn’t enough. Over the years, I’ve learned (and continue to learn) that preparation must be paired with adaptability. Without flexibility, even the best-laid plans can fall apart. I was reminded of this recently when I entered a customer meeting full of ideas for the next phase of work, only to learn they first needed to reassess their priorities before considering anything new. In that moment, all my preparation took a back seat, and adaptability became the real skill that carried the conversation forward.
That balance—being both prepared and adaptable—is what we at TBD Solutions call adaptive preparation. It’s about finding the goldilocks amount of readiness: not too much, not too little—just right.
But how does one do that?
Maybe you tend to be over-prepared and under-adaptable like me. We feel most comfortable with ample time to plan and prepare and to consider all possible scenarios. Too little preparation is the stuff of nightmares for us—it makes us feel anxious and ill-equipped. Our mindset can be rigid and inflexible, and change is hard for us. We’re meticulous, organized, and reliable—but often at the cost of agility. We cling to our plans like life rafts, sometimes to our own detriment.
Or perhaps you’re the type of person who thrives in spontaneity. Adaptiveness is your strength. People like you are often described as flexible, quick-thinking, and resilient in the face of change. You’re comfortable with uncertainty and can pivot easily when things don’t go as expected. But this strength can have a shadow side, too. You may procrastinate or delay getting started because you believe you can always figure it out on the fly. While your improvisational nature can be a gift, it can also lead to missed deadlines, overlooked details, or a sense of being unprepared and scattered.
Regardless of our inclination, the goal isn’t to become someone we’re not—it’s to recognize where we stand and build habits that help us draw from both ends of the spectrum. The over-prepared can benefit from loosening their grip on control and allowing for more flexibility. The hyper-adaptable can benefit from building in more structure and forethought. Growth lives in the middle ground.
Finding that sweet spot of being prepared while being adaptable is challenging, but worth the reward. When we find that rhythm of preparing enough that we feel confident, but not so much that we can’t be nimble, it unlocks the possibility to be great at the work we do and to have fun doing it.
If you find yourself in search of that rhythm, here are some tips to move your needle closer to the middle of the proverbial adaptive preparation spectrum.
Develop a growth mindset.
Expand your comfort zone by learning and trying new things. Seek out learning opportunities by requesting tasks that you have not done before, researching what is new and innovative in your field, or participating in a training. Push yourself to take more risks and view them as a learning experience, don’t expect perfection.
Ask yourself how you can help your future self.
You will thank yourself later for the proactive steps you take now. For instance, schedule time to plan an agenda a week ahead of the meeting. When that day comes, you will be glad you have that time reserved so that step doesn’t get missed or it is no longer feasible to gather key participants. Or create an outline of the brief or training while you’re drafting the proposal or budget. When the time comes to start writing or researching, you will thank yourself for putting thoughts to paper while they were fresh.
Leverage planning tools at your disposal.
Two tools that I love are my Outlook calendar and Asana. An electronic calendar supplies a system for organizing your time. I find it helpful to block time to work on specific tasks and to color-code my tasks by type, such as meetings and project work. This gives me a helpful at-a-glance view of my day and week. Asana, a project management tool, serves to organize projects and tasks. I find this tool to be useful in mapping out the sequence of steps it takes to complete a larger task and in holding people accountable to the tasks and deadlines they are assigned.
Design an environment that supports your goals.
This tip comes from James Clear, author of the popular self-help book, Atomic Habits. Clear proposes that you optimize your environment to make cultivating good habits and avoiding bad ones easy. If your goal is to be better prepared, get yourself a snazzy planner or delete those apps that distract you from focused work. If your goal is to be more adaptable, create opportunities to regularly step outside your comfort zone, try rotating your routines, working in new environments, or taking on projects that require learning new skills.
Seek feedback and learn from it.
Ask a trusted colleague for feedback on an area you want to improve, especially if you admire the strength this colleague has shown in that area. For instance, if you want to be more adaptable, ask for feedback on how you collaborated or responded to questions in a meeting. If you want to be more prepared, ask if your presentation was organized, clear, and concise. Face feedback with an open mind, a willingness to try a new approach, and a desire to be better.
Find that “Goldilocks” amount of adaptive preparation so you feel capable and flexible. Excel in your work—and enjoy the process! When you embrace both organization and adaptability, you’re not just the child craving an orderly and tidy existence; you’re someone who can navigate life’s shifting priorities with confidence and ease.
Author’s Note: This piece was originally written in 2018 based on interviews with Crisis Residential leaders across the country. Some programs mentioned have since changed or closed, but the sentiments, traditions, and insights shared remain an important reflection on the experience of spending the holiday in crisis.
Imagine your favorite holiday memory. What makes it special? Is it belly-laugh hysterical? Or deep with meaning? Does it bring you back to a joyful time in your life? Does it tell the story of love or family connection?
Now imagine what it would take to change this memory into one that was less enjoyable. Think about if Uncle Mark wasn’t there. Imagine if you didn’t get exactly what you wanted for Christmas—perhaps a scooter instead of a bike. Or imagine if the holiday family reunion turned into a bickering session about politics and religion, causing angry family members to leave the party early. Or worse yet, imagine if Dad didn’t make it home in time for Christmas dinner.
All of these unfortunate scenarios pale in comparison to the reality faced by thousands of Americans every year: spending the holiday season away from home receiving mental health treatment. Yet while the circumstances may seem grim, the support offered is often the strongest during these trying times.
Emergency Mental Health Treatment: Crisis Residential Services
There is never a good time to be in crisis, and the holidays are no exception. In these times people experiencing crisis must interrupt their daily lives and celebrations to care for their mental health. For people with depression, anxiety, or psychosis, they may qualify to receive treatment in a more homelike setting than a psychiatric hospital, known as a Crisis Residential Program.
Crisis Residential Programs provide critical mental health treatment in about 600 communities across the United States, offering a safe haven for mental health treatment where people can stay from a few days to a few weeks. Services are often provided in an inconspicuous home within a neighborhood, and clients have access to a psychiatrist, nurses, social workers, and direct support staff. Crisis Residential Programs have a 40-year history of keeping people safe and satisfied while positively affecting their mental health symptoms. These programs often make extensive accommodations to ensure a person feels comfortable, respected, and valued.
Most Crisis Residential homes report high levels of client satisfaction. People who are given access to this treatment option often request it by name if they find themselves in crisis again. Others who have completed their treatment seek out ways to give back through volunteering or employment in a paraprofessional role.
Some Pain is Unavoidable
Even with these considerations, there are virtually no accommodations that can adequately prepare someone to spend the holidays in a residential treatment center. People receiving treatment for addiction or mental illness face these challenges on a regular basis, and some of them lack thoughtful and compassionate family members that include them in their holiday plans.
Even expanded visitation hours and other accommodations can’t completely compensate for being in a Crisis Residential Program during the holiday season. Sometimes people are estranged from their family members and spending a holiday in a crisis home is another variation on a lonely existence. Other people are in a tenuous relationship with their housemates which may have contributed to the current state of crisis, and they are subsequently not welcomed as visitors for the duration of their treatment. Still others are separated by distance or transportation challenges and are not able to be with the ones they love.
Hope in Difficult Times
In response to the challenges faced by clients in treatment, many Crisis Residential providers exhibit compassion and thoughtfulness during this particularly difficult holiday season. Filling stockings, making special meals or food orders, and hosting potlucks are some of the ways the Crisis Residential homes share the seasonal love with the people they serve. Hats, gloves, and blankets are typical gifts provided to clients who reside in colder areas. Practical items like backpacks, journals, and fast food gift cards are also popular gifts. 
Some providers see the value in carrying on traditions with clients or starting new ones. Susan Cromwell, Division Director of Residential Crisis for Mosaic Community Services in Baltimore, MD, believes these efforts are rewarding for clients and staff alike, like taking people to see holiday lights around the city.
Some Crisis Residential homes extend their generosity to former clients of the program, often referred to as “alumni”. At the Harris Center’s Crisis Residential Unit in Houston, TX, alumni are invited to join the clients and staff for a meal and spend the entire day with them. “On December 25th, we always begin with a huge breakfast of tamales, eggs, and breakfast deserts,” says Mende Snodgress, Assistant Deputy of the Comprehensive Psychiatric Emergency Program at The Harris Center. “Later in the day, we have a great barbeque overseen by alumni and staff. We hope to communicate to each of the residents and alumni that they are important members of this family of choice.”
Holidays have presented opportunities for community partnerships between many Crisis Residential homes and churches, grocery stores, and generous donors. At Spring Creek Recovery Center in Sapulpa, OK, they have developed a partnership with a local grocery store that provides a special meal for Christmas, and a local church provides a meal for Thanksgiving.
Some agencies create a budget for holiday gifts and meals for clients, while others simply don’t have the means. In these cases, staff at Crisis Residential homes, like the ones at The Harris Center, contribute money from their own paychecks to ensure the holiday is special for clients.

Many Crisis homes offer special support groups during the holidays to focus on grief, depression, and coping skills during particularly difficult times for clients.
At one Crisis Residential home in west Michigan, staff created an interactive art project called “25 Days of Self-Care”, where, each day, staff and clients create an ornament with a self-care idea attached to it so anyone in the home can engage in healthy behaviors.
Michael Usino, Director at New Perspectives Crisis Services in Pennsylvania, believes that integrating holiday traditions into the Crisis home experience is important for the client experience. “At Hope House and New Perspectives Crisis Services we make every effort to make the holiday—and in particular Christmas Eve and Christmas Day—as ‘normalized’ as possible.” Michael said the house is decorated and clients are welcome to decorate their rooms as well. A Christmas day dinner is provided with collaboration between staff and clients, and families are invited to attend.
The team at Productive Alternatives Crisis Stabilization Unit in Fergus Falls, MN, takes a decidedly different approach. “Since this is a high trauma-triggering season for our clients we keep things quiet and have more neutral seasonal decorations. This can be a highly sensitive time for our people so we don’t place a lot of emphasis on holidays as much as day-to-day and what they can control,” says Beth Nelson, Site Treatment Director at Productive Alternatives. Beth has adopted this approach in part because of her own father’s struggle with bipolar disorder and how the holidays adversely affected him compared to their family and friends.
Productive Alternatives’ approach raises an important consideration: the importance of understanding a client’s emotional relationship to certain holidays and their preferences to celebrate with others or spend time alone or with a supportive staff member. Many clients are open to making new holiday memories despite their condition, and the lengths that Crisis staff go to celebrate the holidays and honor their clients provides a welcome contrast to unfavorable memories of holidays past.
Caring for the Caregivers
Most employers provide a holiday party and gifts for all staff, and some Crisis Residential homes host their own staff parties. Staff are paid overtime for working the holiday (between one and a half and two times their normal pay rate). At Community Research Foundation’s Vista Balboa Crisis Residential home in San Diego, CA, holiday schedules are posted months ahead of time so staff can coordinate coverage with one another. At Continuum Connecticut’s Crisis New Haven home, any holiday time off request is approved, and other supervisory staff fill in the scheduling gaps.
In a season where caring for your clients and your own family’s needs can easily fill the time, one Crisis Residential home’s employees extend their hearts beyond their Crisis home. At the Corinth Crisis Stabilization Unit in Corinth, MS, Helen Rider, Director of the Corinth CSU, says, “We have a nursing home and Animal Shelter Angel Tree and the nursing home gifts are delivered by a staff member on Christmas morning.” She said that staff often playfully argue with one another to determine who will deliver these gifts.
At another Crisis Residential home in Michigan, staff make the most of the holiday celebration by hosting a spirit week where they are encouraged to dress up in festive holiday gear in the week leading up to Christmas. Staff made a full breakfast for clients and each other, including a special Grinch hot cocoa blend (pictured here). 
Some supervisors engage their staff with a holiday door decorating contest, where clients judge the doors and award prizes.
Time Marches On
The holidays have the potential to bring out the best in all of us, even in times of darkness or unwanted struggle. The next time you find yourself enjoying a pleasant, relaxing holiday with the people you care about, remember what a gift it is to be in that place, and consider all the features that make it wonderful. Don’t forget the people spending their holidays in less fortunate circumstances, and think how you could bring hope and beauty to their struggle.

How close has mass violence been to your organization? For some, it’s been assessing unsettling threats; for others, it’s been providing support and care to victims; and for a few, it’s been trying to recover after the unthinkable.
Over the past 25 years, the number of mass violence events and the resulting deaths and injuries have all increased significantly 1. Since the Columbine High School massacre in 1999, more than 420 school shootings have occurred 2.
Some of us don’t just know this upward trend; we can feel it. It manifests as anxiety, fear, and a sense of helplessness of how to make sense of this and what to do.
As a Clinical Consultant who has the opportunity to work with behavioral health agencies across
the country, two questions arise to the top:
The answer to both is yes. Let me tell you how.
For decades, clinical psychology researchers and law enforcement have partnered to develop a behavioral threat ssessment and management literature of evidence-based practice. A standout example from the past 40 years is the Exceptional Case Study Project. Launched by the collaborative efforts of the Secret Service and clinical psychologists, this project was designed to interview and understand assassins.
The Federal Bureau of Investigation’s Behavioral Analysis Unit undertook the study of both mass violence and terrorist mindsets. The Los Angeles Police Department’s Threat Management Unit began a systematic analysis of stalkers and perpetrators of workplace violence. These agencies partnered in large-scale qualitative and quantitative research to understand and help prevent school shootings. Results from this research helped develop a literature that offers both an understanding of the psychology of violence and a framework for effective threat management strategies.
What does this have to do with the behavioral health community? When it comes to violence prevention, behavioral health professionals have something to learn and something to give.
Something to Learn
A common definition of a behavioral health crisis is when an individual is a danger to themself or others. It is typical for violence assessments to consist of a single screening question, “Have you had any thoughts of harming others?”, and intervention is primarily or exclusively hospitalization. Behavioral health crisis providers can learn from the professional threat assessment community’s approach to violence prevention. This approach emphasizes a better understanding, assessment, and intervention when someone is a danger to others.
Something to Give
The professional threat assessment community utilizes behavioral threat assessment and management (BTAM), which directly correlates with the work of behavioral health outpatient and crisis providers. The key parts of BTAM include:
Sound familiar? The behavioral health community brings essential skills and expertise that can significantly strengthen BTAM initiatives.
BTAM is an effective approach, but the real challenge ahead lies in expanding and connecting the network of partners who play a role in it. As behavioral health providers, we have the opportunity to join the BTAM conversations already happening in schools, law enforcement, workspaces, and beyond. By engaging with and learning from the professional threat assessment community, we can deepen our understanding, share our expertise, and stay true to our mission of helping people in crisis. Let’s be a part of setting a new trend.
1 MDI-Mass-Violence.pdf2
2 Examining School Shootings at the National and State Level and Mental Health Implications | KFF

The Community Clinic Behavioral Health Clinic (CCBHC) model provides comprehensive and integrated services to everyone in the community seeking mental health or addiction treatment, regardless of their diagnosis or ability to pay. CCBHCs are required to provide the following nine core services:
CCBHC is not just another funding source for a provider to deliver “business as usual” services. Instead, it is a foundational shift from the traditional behavioral health care methods, which often involved turning away people in need. CCBHCs offer an opportunity to truly transform community-based behavioral health services, embrace a new direction, and provide comprehensive and sustainable health care to everyone.
The CCBHC transformation is not as simple as it sounds, and organizational structures cannot change overnight. Effective change requires education, data reporting, intentional engagement with systems partners, outreach to underserved populations, and understanding of the funding model.
For agencies that embark on the CCBHC journey, the model can dramatically increase access to mental health and substance use disorder treatment, expand a community’s capacity to address the opioid crisis, and improve relationships with essential community resources like schools, hospitals, and law enforcement.
So you want to fully utilize the CCBHC model, what happens first? The initial phase of becoming a CCBHC focuses on a few key factors: implementing core requirements, ensuring evidence-based practices (EBPs) are in place, monitoring key health indicators, developing continuous quality improvement (CQI) plans, and understanding the CCBHC funding model.
Many CCBHCs have evolved from existing behavioral health providers, but the key difference lies in their obligation to serve all individuals and receive funding accordingly. Simply overlaying CCBHC requirements with old service models will hinder the effectiveness of service delivery.
Instead, CCBHCs must seize the opportunity to address unmet community needs by changing operations and expanding service offerings.
The funding structure for CCBHCs shifts away from traditional capitated models and inadequate fee-for-service rates that don’t cover the cost of care. Instead, CCBHCs operate under two Prospective Payment System (PPS) models:
In capitated systems, new service mandates often require providers to reallocate existing resources. CCBHCs, however, can justify funding based on community needs assessments, allowing for strategic investments and the flexibility to proactively develop services for high-risk and hard-to-reach populations.
Real-time encounter and financial data is a necessity for a CCBHC to be effective in implementation, operations, and growth. One way to gather this essential data is through data dashboards specifically designed for CCBHCs to assist with tracking real-time patient encounters, costs, and compliance. Data dashboards also allow help with tracking reimbursements, revenue cycle management, and quality outcomes, all of which are essential for maximizing funding and making data-driven decisions.
A strong needs assessment is essential for justifying services and guiding resource allocation. CCBHCs must identify underserved populations, evaluate existing services, and develop staffing plans and service delivery methods to address gaps. To ensure a comprehensive approach, input should be gathered from diverse community stakeholders.
A well-functioning CCBHC should regularly review its needs assessment, ensuring it incorporates both qualitative and quantitative data from all community partners. For a CCBHC to be effective, it must take its needs assessment seriously, embrace service expansion, and remain vigilant in analyzing data to inform program growth and improve access to care.
One critical, and often overlooked, CCBHC focus area is justice-involved individuals, who experience disproportionately high rates of mental health and substance use disorders. While many providers collaborate with law enforcement through Crisis Intervention Teams (CIT) and crisis response work, equal attention should be given to individuals on probation and parole, where the majority of justice-involved individuals are engaged.
These underserved populations face significant barriers to care, whether transitioning from jail or prison, engaging in treatment, maintaining medications for opioid use disorders (MOUD), or re-engaging after discontinuing MOUD. Parole and probation departments, often burdened with large caseloads, rely heavily on external treatment providers. This population also frequently receives inadequate care due to the combined stigma of substance use disorders, mental health issues, and past convictions. CCBHCs can bridge this gap by developing targeted interventions and expanding services to meet the community’s needs. CCBHCs can play a pivotal role in supporting justice-involved individuals by:
A core goal of a CCBHC is to increase access and engagement for community members. By increasing engagement and individuals coming in for medically necessary services, program revenue increases. Using this revenue, CCBHCs can strategically fund new service lines by maximizing PPS payments, expanding MOUD and behavioral health services with justice involved individuals, and other identified areas of need. However, if a CCBHC does not reinvest earnings to expand and improve care, the PPS rates will decrease exponentially, disincentivizing continued improvements in service access and program expansion. To stay informed on which programs are performing well and which ones need more investment, CCBHCs must monitor all service areas in real time and know how much money can be reinvested into the community.
By fully leveraging the CCBHC funding model, utilizing robust data analytics, and expanding services based on comprehensive needs assessments, CCBHCs can transform community behavioral health care and improve outcomes for the most vulnerable populations.

When I first embarked on my career in psychology, I never imagined it would lead me to work within the prison system. My early days as a therapist were spent guiding teenage boys through the complexities of adolescence—many of whom were navigating the challenges of residential placement due to behavioral issues or histories within the foster care and juvenile justice systems. I was passionate about my work at the agency, but building meaningful dialogue with these young people often felt like a silent struggle. They carried their stories close to their chests, making the therapeutic process a delicate dance of patience and persistence.
Despite the challenges, I found immense value in my role as a psychologist—listening to people, thinking about and helping solve problems, being part of a community of like-minded professionals, and having many opportunities to learn. Counseling gave me the rare privilege of truly seeing who people are and helping them bring their best selves forward. I witnessed profound transformations: kids reunited with their families, individuals putting substance abuse behind them, and clients replacing harmful habits with healthier lifestyles. One of the most important lessons I learned was that therapy isn’t just about aha moments—it’s about relationships with others and making steady, intentional steps toward change. During this period of introspection, an unexpected opportunity arose—a call from the Department of Corrections inviting me for an interview. Initially, I was hesitant, but curiosity led me to explore this new avenue.
A New Chapter: Stepping into the Unknown
Walking into a Michigan prison for the first time was an experience filled with mixed emotions of nervousness and anticipation. The warm, inviting counseling offices and family-oriented environments were replaced by razor wire-adorned fences, security gates, and rooms with mismatched, severely worn office chairs. Distrustful eyes followed me as I moved through the facility, a reminder that this was a world governed by suspicion and control. Adapting to this environment required personal resilience and the support of those who had walked this path before me. The transition was challenging, but within these challenges, I found surprising growth.
Breaking Stereotypes: What Prison Really Teaches Us
Looking back, it’s clear that each step has shaped me both personally and professionally. One key lesson I’ve learned is that prison isn’t what you see on television. While TV often compresses events into an hour of constant drama and violence, the reality is far more nuanced.
Yes, prison can be a place of despair and trauma, but it can also be a place of hope and transformation. From the outside, we tend to focus on its punitive nature. However, there are individuals inside who are actively working to change their trajectories, learning new skills, and adapting how they relate to others in positive ways.
The Power of Patience in Bureaucracies
Change can be slow in governmental bureaucracies, but with persistence and patience, I was fortunate enough to contribute to and witness numerous positive initiatives. While many of these efforts took months or even years to come to fruition, collaboration was the driving force behind their success. I worked alongside state departments, private organizations, and dedicated volunteers to improve systems and outcomes for both incarcerated individuals and the staff who support them.
One area of progress was expanding mental health and substance use disorder treatment programs. I participated in efforts to enhance access to these services, ensuring that incarcerated individuals received evidence-based care that could help them address underlying issues and reduce recidivism. Re-entry services also became a priority, which helped prepare individuals for life beyond prison walls by equipping them with the necessary tools to succeed in their communities.
On the clinical side, I contributed to improving practices such as suicide risk assessment and group therapy facilitation. These changes not only improved the quality of care but also supported staff by providing them with better tools and training to navigate complex situations. Additionally, I was involved in addressing the overuse of restrictive housing (solitary confinement) and advocating for alternative approaches that emphasized rehabilitation over isolation.
Prison systems can be both surprisingly progressive and surprisingly outdated compared to life outside the fences. For example, while everyone in prison has equal access to healthcare—a stark contrast to many underserved communities—there are still significant gaps in technology and infrastructure that require innovative solutions.
These experiences taught me that meaningful change is possible when people come together with shared goals and a commitment to progress. While the process often tested my patience, it also reinforced my belief in the power of persistence and collaboration.
Unsung Heroes: The Corrections Staff
Corrections staff work is often thankless and goes unnoticed by the general public. Yet, behind the razor wire and locked gates are thousands of professionals who dedicate themselves to maintaining community safety while supporting the well-being and rehabilitation of incarcerated individuals.
From officers who take time to de-escalate tense situations with patience and understanding, to counselors who help individuals confront a lifetime of trauma, these professionals embody what it means to serve others under challenging circumstances.
Corrections staff are also instrumental in driving systemic change. They implement new training on trauma-informed care or evidence-based interventions, often rethinking long-standing practices to better serve both incarcerated individuals and their colleagues. Their willingness to adapt and grow has been pivotal in creating safer, more rehabilitative environments within the system.
Corrections staff are not just enforcers; they are mentors, mediators, and advocates working within a system that offers little recognition for their efforts. They witness some of society’s most difficult realities while striving to create an environment where growth and change are possible.
Challenging Misconceptions: A Call for Change
It’s time we challenge some deeply ingrained beliefs such as “people who commit crimes can’t change” or “harsh punishment is an effective deterrent,” which have contributed to making the U.S. the most incarcerating nation in the world. We must also confront misconceptions about addiction being a moral failing or mental illness equating to danger.
Throughout my journey in corrections, I’ve been inspired by countless success stories and transformative programs within the prison system. My focus areas have evolved over time: improving transition processes for those leaving incarceration, addressing Adverse Childhood Experiences (ACEs), promoting trauma-informed care, advancing evidence-based treatments for mental health and substance use disorders, and enhancing suicide prevention efforts within justice settings.
A Vision for True Safety
Reflecting on my unexpected path into corrections has reinforced one truth: true safety comes from addressing root causes like inadequate healthcare access and untreated mental health issues. If we want safer communities, we must break cycles of recidivism by fostering rehabilitation over retribution.
Achieving this paradigm shift requires a collective societal effort to challenge misconceptions about incarceration, combat stigma surrounding mental health issues, and support those affected by these systems. By embracing compassion alongside evidence-based practices, we can move beyond fear towards a more rehabilitative approach.
Join Me in Advocating for Change
The road ahead is challenging, especially in the face of a shifting political climate that may not be friendly to reform efforts. Now more than ever, we must stay committed to advocating for a justice system that values healing over punishment.
I invite you to join me on this journey towards meaningful reform—whether through advocacy for policy change, supporting programs that promote rehabilitation, or simply challenging misconceptions in your community. Together, we can push back against regressive policies and build a society that believes in second chances and works toward breaking cycles of harm for good.
What is a Care Pathway?
A care pathway is a multidisciplinary plan of care that outlines the sequence and timing of interventions for patients with particular conditions or undergoing specific procedures.1 Care pathways help to ensure that persons served2 receive the appropriate intervention, rooted in best practices, through the standardization of clinical processes. Care pathways clearly define treatment parameters, promote interdisciplinary team-based care, and provide ongoing monitoring to assess the effectiveness of the care pathway.
Defining and implementing care pathways is essential for healthcare providers. A care pathway aims to increase the quality of services and improve outcomes while employing a patient-centered approach to care. For example, does the care pathway help reduce the risk of addiction for a certain population demographic? Care pathways provide clear, consistent guidelines and help staff adapt quickly and perform effectively. When care pathways are well-defined, they can effectively evaluate outcomes such as a reduction in risk, a decrease in symptoms, or an improvement in quality of life. To measure a care pathway’s impact, it is crucial first to define the pathway and its intended goals.
What a Care Pathway is Not
Many concepts in healthcare are used interchangeably with care pathways but vary slightly in meaning. It is important to identify and define these associated terms to ensure consistency in terminology and construct.
Characteristics of a Care Pathway
Care pathways must include a standard set of features or attributes to achieve their purpose. Care pathways must be:
Components of a Care Pathway
Care pathways can range from simplistic, encompassing just a few targeted activities within a single interaction, to complex workflows involving a multidisciplinary team spanning a broader episode of care. Regardless of the complexity, every care pathway should encompass the following:

Implementing a Care Pathway
After understanding the purpose of a care pathway, implementation is the next step. To implement care pathways in healthcare settings, follow the seven steps listed below.
Step One: Identify
The population a care pathway supports can be defined in various ways, including by diagnosis, demographics, or social determinants of health (SDoH). Regardless of the criteria, identification must be systematic and documented well. For instance, a care pathway for individuals with schizophrenia on antipsychotic medications must reliably identify active diagnoses and prescriptions. Additionally, stratification within the subpopulation may be necessary if interventions differ based on factors, such as symptom severity, level of need, or service utilization. Stratification is only necessary if it leads to different interventions based on the categories.
Step Two: Research
Once the target population is identified, a systematic review of best practices is essential. This includes researching appropriate screening tools, evidence-based practices, clinical guidelines, and protocols to inform the care pathway. Some methods, such as Screening, Brief Intervention, and Referral to Treatment (SBIRT), and Motivational Interviewing (MI), may be applicable across multiple care pathways.
Step Three: Define
The next step is to synthesize the findings from the systematic review and define the care pathway, documenting the ideal clinical workflow. This includes identifying each activity and clearly defining roles and responsibilities. When responsibilities shift between staff or departments, a well-defined pathway ensures a seamless transition.
Step Four: Map
This step involves identifying existing components of the care pathway and determining how to transition from the current to the ideal state. A key part of this gap analysis is understanding how each pathway element will be documented and tracked in the electronic medical record (EMR). Key considerations include:
Consult EMR vendors, clinics, and healthcare consultants to learn from similar implementations. Based on the gap analysis, develop an implementation plan outlining the phased steps required to move toward the ideal state.
Step Five: Implement
Using the implementation plan as a roadmap, organizations can begin developing the care pathway, considering timelines and dependencies for each phase. Adjustments may be needed if certain steps take longer than expected, but incremental progress is still moving toward the ideal state. Since training is critical to successful implementation, consider creating a companion guide for staff with detailed instructions, talking points, and additional resources. Depending on the pathway’s scope, it may be beneficial to start implementation in a specific program or department, with expansion in later phases as processes and protocols are refined.
Step Six: Refine
A care pathway should be flexible, adapting as best practices evolve or organizational changes occur. Once implemented, the care pathway should be monitored to ensure each component functions as intended. Key questions to consider include:
Adjustments should be made as needed to ensure consistent positive outcomes.
Step Seven: Evaluate
The final step is developing a plan for evaluation considering the outcomes of persons served. Look for answers to questions like, does the care pathway reduce risk, decrease symptoms, or improve quality of life? Developing clear measures and benchmarks is one way to understand the impact of implementing the care pathway.

The name Ruth Wakefield is not likely one that you recognize, but you most certainly know the invention she is credited for.
Ruth and her husband Kenneth owned a toll house in Whitman, Massachusetts in the 1930’s. Toll houses operated in the 1700-1800’s, serving not only as a building for which to collect tolls, but also as a haven for travelers to rest and enjoy a home-cooked meal. Ruth and her husband converted their toll house into a lodge, naming it the Toll House Inn.
True to the tradition of serving home-cooked food, Ruth baked for guests of the Inn. One of her favorite recipes to make was the Butter Drop Do cookie, and one day while she was making them, she decided to mix up the recipe by breaking a Nestlé chocolate bar into bits and adding them to the cookie. The delicious result was a cookie with soft, creamy chocolate morsels. Her recipe gained fame at the Inn and found its way into regional newspapers, exploding the sale of Nestlé chocolate bars.
Ruth’s innovation of tiny pieces of chocolate led to the creation of packages of chocolate morsels, or what we have come to call chocolate chips1.
Innovative ideas, like the chocolate chip, don’t always come from those in senior positions. Great ideas can—and should—come from those doing the work, like the baker. In behavioral healthcare this means that CEOs, directors, supervisors, and managers don’t possess all the solutions to the challenges their workforce faces. As leaders our charge is to empower direct care workers, peer support specialists, case managers, nurses, and other frontline workers to leverage their knowledge, experiences, and perspectives to challenge the status quo, make work easier, and serve people well.
To empower innovation on your team, consider the following:
Ruth was able to create the chocolate chip because she was directly involved in baking for the Toll House Inn. Because she was directly involved, she could see the challenge and solution to making Butter Drop Do cookies. Ruth was also empowered to try new ideas, free to explore cutting a chocolate bar into tiny pieces to see what would happen. And finally, Ruth had the time and resources available to set aside her other responsibilities and dedicate her attention to perfecting her recipe.
Direct involvement in the day-to-day work, empowerment, and the gift of time and resources are the recipe for innovation for frontline workers. Consider ways your program can bring innovative ideas to fruition through a thoughtful process, friendly competition, or the broadcasting and celebration of innovation.
*The invention of chocolate chips story was adapted from the History of Nestle Toll House.

Is your program required to undergo a program audit or quality site review? If so, it’s likely that just the term “audit ” creates an emotional reaction. Audits can seem like a disruptive annoyance, a “gotcha”, or a procrastinator’s nightmare, but it doesn’t have to be. Like most things, preparation is key. If you and your team are organized, understand the standards, have been keeping good records, and maintain audit readiness throughout the year, your experience may even be positive, and those auditors will be in and out in no time.
The American Society for Quality (ASQ) defines auditing as the on-site verification activity, such as inspection or examination, of a process or quality system, to ensure compliance to requirements. Auditing can also be done virtually or via a desk audit, where items are submitted for review to an auditor. Regardless of how you define auditing, everyone seems to dread an audit. Audits seem to raise a level of anxiety among people even if they believe they are following the “rules”. It does not seem to matter if the audit is internal or from an external entity, no one likes the “gotcha” experience and everyone wants to put their program in the best possible light.
Over the years,I have participated in many program audits. I have also conducted many audits and program reviews. Based on almost 30 years of experience, I have found the following activities not only prepare an organization for an audit but reduce the dread and anxiety that audits produce.
Get organized. Look at a calendar and determine how much prep time you have. Even with very short notice, you can successfully prepare for an audit. Obviously, the amount of time you have will dictate if this is an all-hands-on deck type of preparation or if you have time to thoughtfully divvy up tasks. Review all the information sent to you about what to expect from the audit and what will be required of you. Many times, audit notifications include specific documents that must be gathered, a calendar of activities or topics, individuals to be interviewed, etc. It is also a good idea to review previous audit reports including any corrective action plans that were implemented. Auditors will want to see evidence of those activities and ensure you have sustained improvement in those areas.
Review the standards.Take a good look at what will be reviewed. Standards may be outlined in a manual, in statute, in a contract, on a website, or provided in an auditing tool that will be used by the auditors. It is important to not only review the standards but understand their intent – “The spirit of the law”. By understanding the intent of the standard, you can identify the many areas one standard might involve. For example, a clinical program standard may require a signed consent on file. The intent of that consent is to inform the individual of the risks and benefits of the treatment prior to the provision of services. A signed consent does not meet the standard if it is signed after treatment begins or does not include a description of the risks and benefits of the treatment.
Identify your team.An audit should always be a team effort. It is a great way for staff to learn about the standards and how your organization’s policies and procedures are designed to meet the requirements. It is also a great way for staff to take ownership of their work. Lastly, participating in audit preparation can help individuals understand why certain things are in place. Have you ever had a staff person ask why a certain question is on an assessment or why you must do things a certain way? Most likely it is due to a standard or previous audit finding.
Collect evidence of compliance.Once you are familiar with the standards, begin collecting evidence that supports compliance with each requirement. Evidence may include policies and procedures, training records, clinical documentation, data, etc. Building this physical or electronic “proof box” of documentation is an essential part of being prepared and demonstrating your program’s compliance.
Conduct a gap analysis.Identify which areas you lack evidence of compliance, or areas where your evidence of compliance is not strong. It is always best to anticipate these areas and self-identify standards in advance where auditors may not find evidence of full compliance.
Develop a plan.If there is time, it is always best to attempt to obtain evidence of compliance or steps that are actively being taken towards meeting the standard. There are, however, some items where evidence just does not exist or is lacking. In those cases, the best way to address the lack of full compliance is to develop an improvement plan. An improvement plan can be implemented immediately and will demonstrate to the auditors that you are taking action to correct the issue. You may still be cited, but you will be proactive rather than reactive.
Conduct a mock audit. A mock audit is a great way to assess those areas that are not easily demonstrated through documentation. Mock audits can provide a realistic sense of policies and procedures in action and program staff’s knowledge and understanding of the standards. Mock audits can give you a true sense of what is or is not occurring in the program, offering the opportunity to interview staff, answer questions, and provide feedback.
Create an audit-ready culture.Creating the right culture is probably my most important tip. Coaching your program team to understand the standards, keep documentation up-to-date, and be “audit ready” year-round makes the actual audits less of a heavy lift and less anxiety-provoking. Audits can then be viewed as an opportunity for your program to shine!
We need innovative solutions to the mental health problems our communities are facing. How do we respond to increasing rates of depression and anxiety, the overuse of emergency rooms for mental health care, high rates of death by suicide and drug overdose, and budgets that never seem to cover what’s needed?
I’ve spent years facing these problems, yet I haven’t spent nearly as long considering the question that makes solving the problems possible: How does innovation happen?
I used to think innovation was the result of creative people’s spontaneous thinking. Imagine Alexander Graham Bell inventing the telephone by casually walking down the road and shouting, “Wait! Why walk to deliver this message on foot when I could transmit my voice through vibrations and current over wire!” Viola! Spontaneous innovation.
When I began reading the biographies of great innovators, however, I found they took a different approach. Leonardo Da Vinci transformed art not by obsessing about its current limitations, but by dialoguing with disciplines outside of art. Leonardo studied anatomy and the muscles that move lips to craft the world’s most intriguing smile. He talked with scientists about light, optics, and geometry to lead the Renaissance innovation of dimensionality in art. This was the spirit of the Renaissance, to learn broadly across disciplines and innovate through connection.
Four hundred years after Leonardo, Robert Oppenheimer led the Manhattan Project in pioneering the era-defining innovation of nuclear fission. He did this by the Renaissance method of finding connections in diverse ways of thinking. Growing up, Oppenheimer loved reading the classics in Greek and Latin, reflecting on French poetry, and admiring Dutch art. He continued this practice of absorbing diverse information and finding connections as a theoretical physicist and leader. In the daunting task of resolving the constant scientific arguments during the Manhattan Project, Oppenheimer was famous for listening to both sides, pointing out connections in the diverse ways of thinking, and thus illuminating a way forward.
In today’s age of unbelievable information and connection potential, the key ingredient now is the will to learn broadly across disciplines. For mental health innovation, what Renaissance connection is out there waiting for us? Here are a few promising directions I’ve seen:
Our communities need innovative solutions when facing mental health problems. Instead of waiting for a spontaneous innovation, we can listen to those outside of mental health and find the connections for the way forward. Let’s follow the Renaissance path, blazed by those who have changed the world.
Book References:
Leonardo Da Vinci by Walter Isaacson (2017).
American Prometheus: The Triumph and Tragedy of J. Robert Oppenheimer by Kai Bird and Martin Sherwin (2006).

Do you remember the moment you fell in love with your work?
For me, the most fulfilling experience of my career in
behavioral health care involved supporting and designing crisis
residential units1, or CRUs, across the state of Michigan. New
to the field as a macro social worker, I was privileged to be
considered a subject matter expert in CRUs by my peers. Soon
after, I was tasked with designing and opening a CRU in
Michigan’s Upper Peninsula, a project that brought me great
excitement and honor.
At the time, I knew little of the U.P., aside from its identity as a
winter wonderland far from home. I was committed to
designing and opening a CRU that met the needs of the U.P.
community, and I made it my mission to get to know the
extremely rural portion of my beloved state over several
months. This meant becoming a veritable dual citizen of the
upper and lower peninsulas of Michigan. Little did I know, this
dedication allowed me to avoid an incredibly prevalent
misstep in crisis services design and planning- plugging in a one-size-fits-all solution.
One-size-fits-all, or even one-size-fits-most, is a fallacy. A behavioral health crisis program or continuum
may appear to fit a community, but that does not mean it fits well. When the default is a one-size-fits-
all approach without considering the unique needs of a community, a mismatch or gap occurs and
complications can arise in our relationships where trust begins to erode, and doubt takes over.
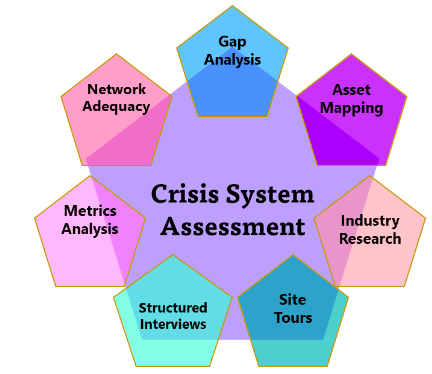
Crisis services are in the midst of a long-awaited and well-deserved spotlight. Thoughtful and sound research blended with the development of tools are advancing and expanding crisis system knowledge rapidly. While increasingly accessible tools inform the development of strong crisis services, no one tool is the golden goose. It would have been a grave mistake for me to assume that a program that found success serving Kent County, Michigan (population 658,046) would realize the same success serving all the Upper Peninsula (population 301,609 but 18 times larger in area). In population density alone, the differences paint a clear picture.
As you engage dialogue and planning for crisis service development and expansion in your community, consider what makes it unique. Do you live in a college or university town? Is your funding system complex and nuanced? Is the geographic location urban, suburban, rural, or frontier? Is there good access to public transportation, or have the tires of an Uber never touched the roads? Through thoughtful assessment and community engagement, the rightsized behavioral health crisis continuum can be developed in any community.
1 Crisis Residential Units are short-term behavioral health treatment programs in which individuals experiencing a behavioral health crisis receive person-centered care in a 24/7, homelike setting.



